Dr James Fallon, Brighton and Sussex Medical School
Substance misuse tutorial
This tutorial will cover the following:
- The features of dependence
- Withdrawal features of alcohol, opiates and benzodiazepine
- The management of alcohol withdrawal and appropriate benzodiazepine regimens
- B1 deficiency physical complications of this
- The management of opiate withdrawal and appropriate management
- Non-pharmacological interventions in substance misuse
The features of dependence
The DSM criteria for dependence can be easily remembered with the acronym “WITHDraw IT“:
3 of 7 within 12 month period:
Withdrawal
Interest or Important activities given up or reduced
Tolerance
Harm to physical and psychosocial known but continue to use
Desire to cut down, control
Intended time, amount exceeded
Time spent too much
N.B. Physical withdrawal is not necessary for a diagnosis of dependence
Alcohol Dependence
Withdrawal symptoms
Additional notes
Don’t forget that in tolerant drinkers withdrawal can occur despite a high Blood Alcohol Content i.e. just because they blow a high reading on an alcometer doesn’t mean they don’t require treatment – the decision to treat should be done on an individual clinical assessment not an alcomenter reading.
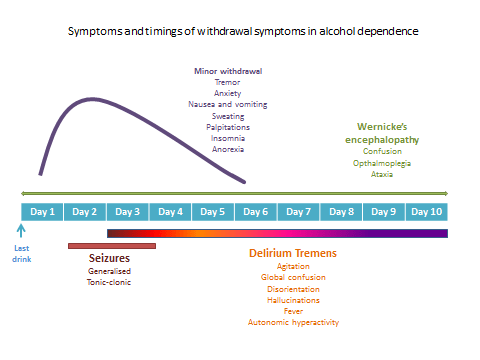
Minor withdrawal
Begins around 8 hours after a significant fall in blood alcohol and will worsen until peaking on day 2 of abstinence.
Delirium tremens
Most commonly begins in the first 2-3 days of abstinence. The hallmark is global confusion so don’t forget this as a possibility when doing a delirium screen or if a patient suddenly becomes agitated on the ward several days post admission.
Seizures
Seizures are the primary concern with acute alcohol withdrawal, should these occur with an inpatient then management with PR diazepam is appropriate. They tend to occur later in the presentation, normally 24-48 hours after stopping alcohol use and are generalised tonic-clonic in nature.
Ensure you take a full seizure history in those who report a history of withdrawal seizures as non-professionals will often describe a variety of experiences such as syncopal blackouts as fits or seizures.
Immediate management of severe withdrawal symptoms
| Minor withdrawal symptoms and prevention of seizures and DTs | Reducing regimen of benzodiazepine |
| Generalised tonic-clonic withdrawal seizure | Diazepam 10mg PR |
| Delirium tremens | Lorazepam 2mg PO 2nd line – lorazepam 2mg IM for management of agitation |
Management of alcohol dependence – detoxification
There are two options for detoxification:
- Community detoxification –
- Mostly under the supervision of specialist community alcohol services (some GPs will also provide this service)
- Inpatient detoxification:
- In a specific specialist detoxification ward
- As part of a hospital admission for a medical problem during which alcohol dependence is found on history
As a general rule general hospital admissions for a patient who presents to A&E wanting an admission for detoxification are not advised. This is for several reasons, mainly that whilst the medical detox is relatively straightforward the maintenance of abstinence in the community is much more difficult and requires the support of different services. As such it is advised that detoxification is done by a specialist substance misuse service who will be able to assess for suitability, work on building resources prior to admission and (hopefully) put a robust plan for the post-discharge period.
Scientific basis to withdrawal management
For a brilliant one minute (genuinely) guide to this process see One Minute Medicine’s video:
So in withdrawal neurons are in a hyper-excitatory state due to down regulation of GABA and the sudden withdrawal of alcohol to have an action on the remaining receptors (inhibitory receptors) so we need to have a replacement drug that acts on GABA receptors. Luckily we have benzodiazepines which do just this and we reduce them in a step wise fashion.
In the benzodiazepine REDUCING REGIME one of two drugs are usually used
- diazepam
- chlordiazepoxide (NICE recommended due to lower risk of abuse)
The decision is usually made by the trust at which you are working who will provide a very handy template for you.
| Drug name and route of administration: Diazepam PO |
| High start | Medium start | Low start | |||||
| Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 6 | Day 7 | |
| Date | |||||||
| 8 am | 20mg | 20mg | 15mg | 10mg | 10mg | 10mg | |
| Signed | |||||||
| 12 pm | 20mg | 15mg | 15mg | 10mg | |||
| Signed | |||||||
| 5 pm | 20mg | 15mg | 15mg | 10mg | 10mg | ||
| Signed | |||||||
| 10 pm | 20mg | 20mg | 15mg | 10mg | 10mg | 10mg | 10mg |
| Signed | |||||||
| Prescribed by : | Name | Signature | Date |
This leaves you just to select the appropriate dosing, which you will do on the basis of daily alcohol consumption along with their risk of seizures or delirium tremens.
N.B. This should be reviewed daily for the first few days to determine if the patient will require a longer detox period, you will see this if they are using lots of prn medication. You can then titrate the dose up and begin reducing again.
Those with prominent withdrawal symptoms, comorbid benzodiazepine dependence or very high alcohol intake (over 50 units daily) will be likely to require a longer detox period with an extended reducing regimen.
There will also be space for prn medication for breakthrough withdrawal symptoms:
PRN Medication for breakthrough withdrawal: Diazepam PO 10-20mg
| Date | ||||||||||
| Signed |
| Prescribed by : | Name | Signature | Date |
With a space for PR diazepam in the event of seizure.
Vitamin supplementation
In all patients who are alcohol dependent vitamin supplementation should be given, both for those who are drinking dependently in the community and those undergoing detoxification.
Oral vitamins should include (dosing recommendations may vary a little between different trusts):
- Thiamine 100mg tds
- Vitamin B co-strong ii tds
- Multivitamins i od
In hospital vitamin supplementation is via parenteral thiamine (Pabrinex).
B1 (Thiamine) deficiency and related physical complications
The most serious consequence of thiamine deficiency is Wernicke’s encephalopathy which can progress to Korsakoff’s syndrome.
Why are alcohol dependent patient deficient in thiamine?
For two main reasons:
- Inadequate intake
- due to poor diet – this is the primary reason for deficiency
- Malabsorption of thiamine due to
- impaired absorption of thiamine from the gut,
- impairment of storage by the liver
- though in those with adequate intake of B1 it would be unlikely that the patient would be deficient
Why does brain damage occur?
Think back to the Kreb’s cycle – how cells generate energy.
Thiamine plays a role in carbohydrate metabolism, it works as a cofactor for several enzymes in the Krebs cycle so when deficient there is a failure in those thiamine dependent cellular systems. This leads to cell death. Unfortunately for alcohol dependent patients thiamine dependent enzymes have a key role in cerebral energy utilisation so there can be cell death in the brain when thiamine is deficient.
Keeping it simple – thiamine deficiency leads to cerebral cell death, mostly in these areas:
Full paper: https://pubs.niaaa.nih.gov/publications/arh27-2/134-142.htm
IV fluids and dependent drinkers:
The risks relate to thiamine deficiency and can be summarised as:
DO NOT GIVE IV DEXTROSE
Glucose oxidation uses a lot of thiamine, which can precipitate Wernicke’s encephalopathy if a patient is thiamine deficient due to the increased demand for thiamine from this glucose oxidation.
It is also good practice to ensure that with alcohol dependent patients are given IM or IV thiamine supplementation prior to eating for the same reason.
Symptoms of Wernicke’s encephalopathy
The classical triad of this disorder is:
- Confusion
- Opthamoplegia
- Ataxia
However, it will commonly (around 90% of cases) present without all three symptoms and is underdiagnosed.
Prevention and treatment of Wernicke’s
The use of thiamine is essential in all detoxifying alcohol patients. For those suitable for community detoxification, who will be at a lower risk for the disorder, this may be appropriately done with high dose oral thiamine.
However, for those managed on an inpatient unit, either a specialist detoxification unit or a general hospital then parenteral thiamine (Pabrinex) should be used. Depending on the unit you work at this may be given IV or IM. Doses range depending on unit and there is no general consensus on what the best dosing regimen is but NICE recommend 5 days treatment as a minimum. (this will usually be on the detoxification template)
Progression to Korsakoff’s
N.B. This is at times referred to as Korsakoff’s psychosis, but as the disorder is not psychotic in nature it is now generally referred to as Korsakoff’s syndrome or Korsakoff’s amnesiac syndrome.
For a patient with Wernicke’s encephalopathy the use of parenteral thiamine may reverse many of the problems and prevent conversion to the long term condition known as Korsakoff’s syndrome.
However, for a proportion this will develop and will present as:
- Persistence of any Wernicke’s symptoms such as ataxia
- Confusion, which will present as CONFABULATION, this is characteristic of the condition and can be thought of as a filling in of the gaps in memory. As such a patient may present quite well but their responses to the same questions when asked at another time may change or may not be based in reality, they can sometimes be bizarre in nature.
- Antereograde amnesia – the inability to make new memories
- Retrograde amnesia – the loss of some memories prior to the development of the disorder
Benzodiazepine dependence
As benzodiazepines work on GABA receptors the symptoms and management are largely similar to that of alcohol. The main differences are that thiamine deficiency and thus Wernicke’s/Korsakoff’s are less likely to be an issue and that the detoxification is likely to take longer, around 2 weeks on an inpatient unit.
As testing for benzodiazepines is via urine drug screen and the treatment in detoxification is benzodiazepines community treatment is fraught with complication for those with a dependence on illicitly obtained benzodiazepines as one can never be certain that there is not use on top. As such the decision to provide a community detox is not taken lightly.
Withdrawal symptoms
- Recurrence of original disorder.
- Rebound symptoms – last a few days.
- Withdrawal syndrome
- increased anxiety, tremor, irritability, restlessness, dizziness, sweating, insomnia, nightmares
- Serious symptoms
- seizures, delirium, confusion.
- Other symptoms
- anorexia, nausea, tinnitus, excessive sensitivity to light and sound, depersonalisation and derealisation.
